
Smallpox vaccination implications for orthopoxvirus susceptibility
Published:
An overview of our paper: “The global landscape of smallpox vaccination history and implications for current and future orthopoxvirus susceptibility: a modelling study” published in The Lancet Infectious Diseases.
My coauthor, Dr. Shweta Bansal, previously shared this thread on Twitter and I have updated and archived it here.
The 2022 mpox outbreak brought to the forefront the legacy of smallpox eradication. Historical smallpox vaccination efforts were heterogenous leaving a modern patchwork of long-lasting protection. We characterized this landscape in this project.
History
In 1967, WHO initiated an intensified smallpox eradication campaign. The target was 80% vaccination coverage everywhere, but the bifurcated needle stretched stocks and ring vaccination efficiently decreased transmission leading to earlier elimination at lower vaccination coverage in each country.
By the time WHO declared smallpox eradicated in 1980, there was a geographically heterogeneous layer of protection against smallpox worldwide. After eradication, smallpox vaccination was ceased everywhere by the mid-1980s but the cessation date varied.
Why do we care now?
Mpox, another orthopoxvirus, like smallpox, is spreading in over 70 countries. At the same time, other zoonotic orthopoxviruses are increasing. But the great news? The smallpox vaccine is expected to be highly effective against mpox & other orthopoxviruses
So where is smallpox vaccine protection found globally, you ask? This is not comprehensively known. So, we put together a database based on historical and current information.
Important pieces:
- When was smallpox vaccination stopped in each country + how many were vaccinated before then?
- The expected effectiveness of the smallpox vaccine against mpox + other orthopoxviruses
- The current age distribution of the population within each country
These factors vary geographically based on historical public health efforts and modern demographic trends.
What did we find?
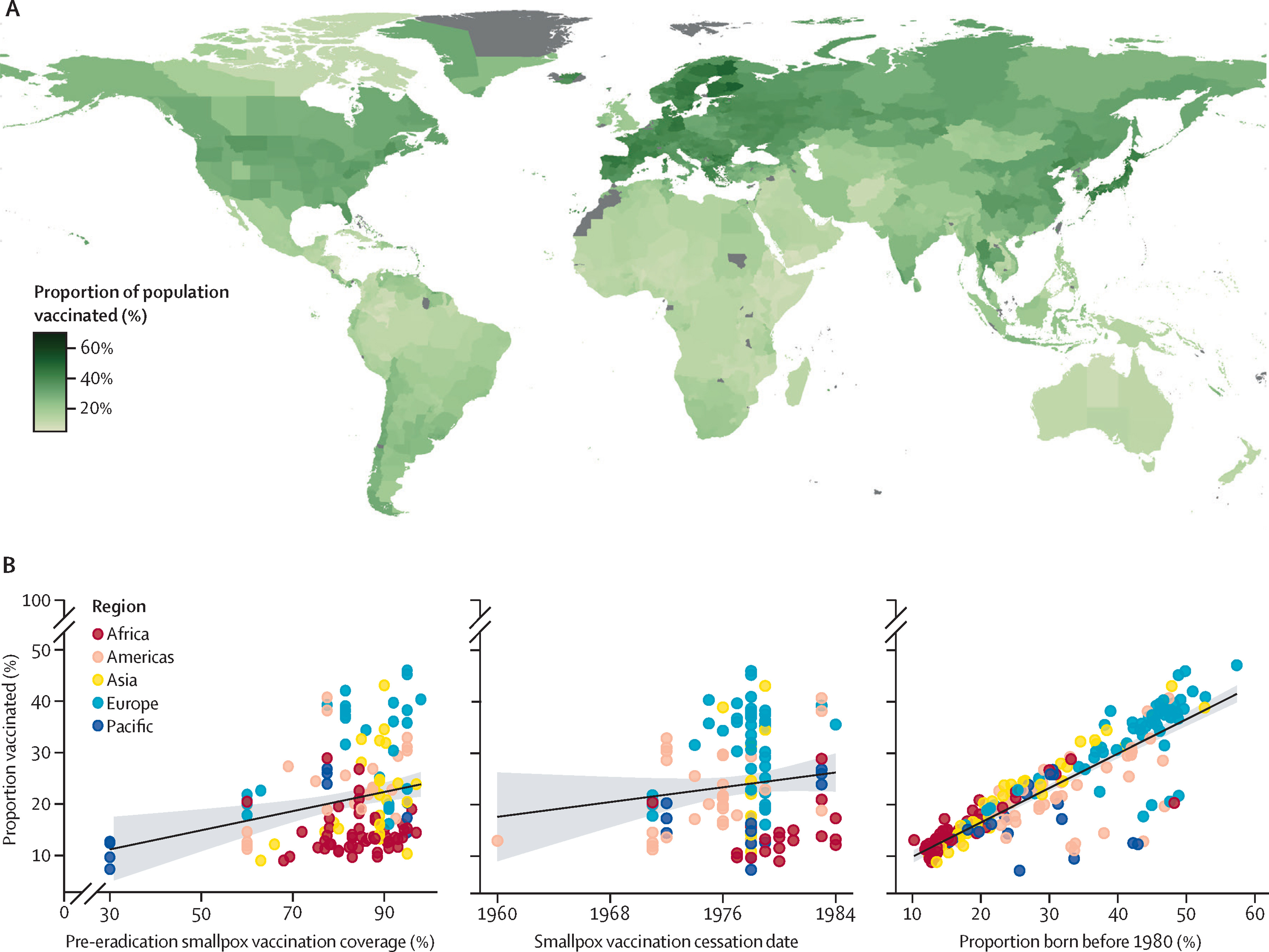
Putting this all together, we create a high-resolution global map of current population smallpox vaccination coverage, accounting for the distribution of smallpox vaccination & demographic changes post-eradication. At least 50% of the population of any region is not vaccinated for smallpox and therefore susceptible to mpox as of 2022, but variation abounds.
Given the pieces that make up these susceptibility distributions, you might wonder: what’s most important? We find that current demography is highly predictive: younger populations have lower smallpox vaccination coverage are thus more susceptible to mpox. For places with older populations, past smallpox vaccination coverage levels are also relevant.
More data is available for the US, so we can look at US smallpox vaccination coverage at a finer scale accounting for heterogeneous vaccination coverage within the country and demography. We also consider US immigration – since non-US-born people may have been vaccinated later than 1972 (when the US stopped smallpox vaccination).
Takeaways
There is a distribution of substantial global protection against orthopoxvirus diseases. But there is significant geographic variation in susceptibility, at national and subnational scales, driven primarily by demographic changes since smallpox eradication.
How does this help? In the event that mpox transmission becomes widespread, this map can inform public health efforts on assessing risks of geographic introductions & scarce vaccine supply allocation.
Nuances
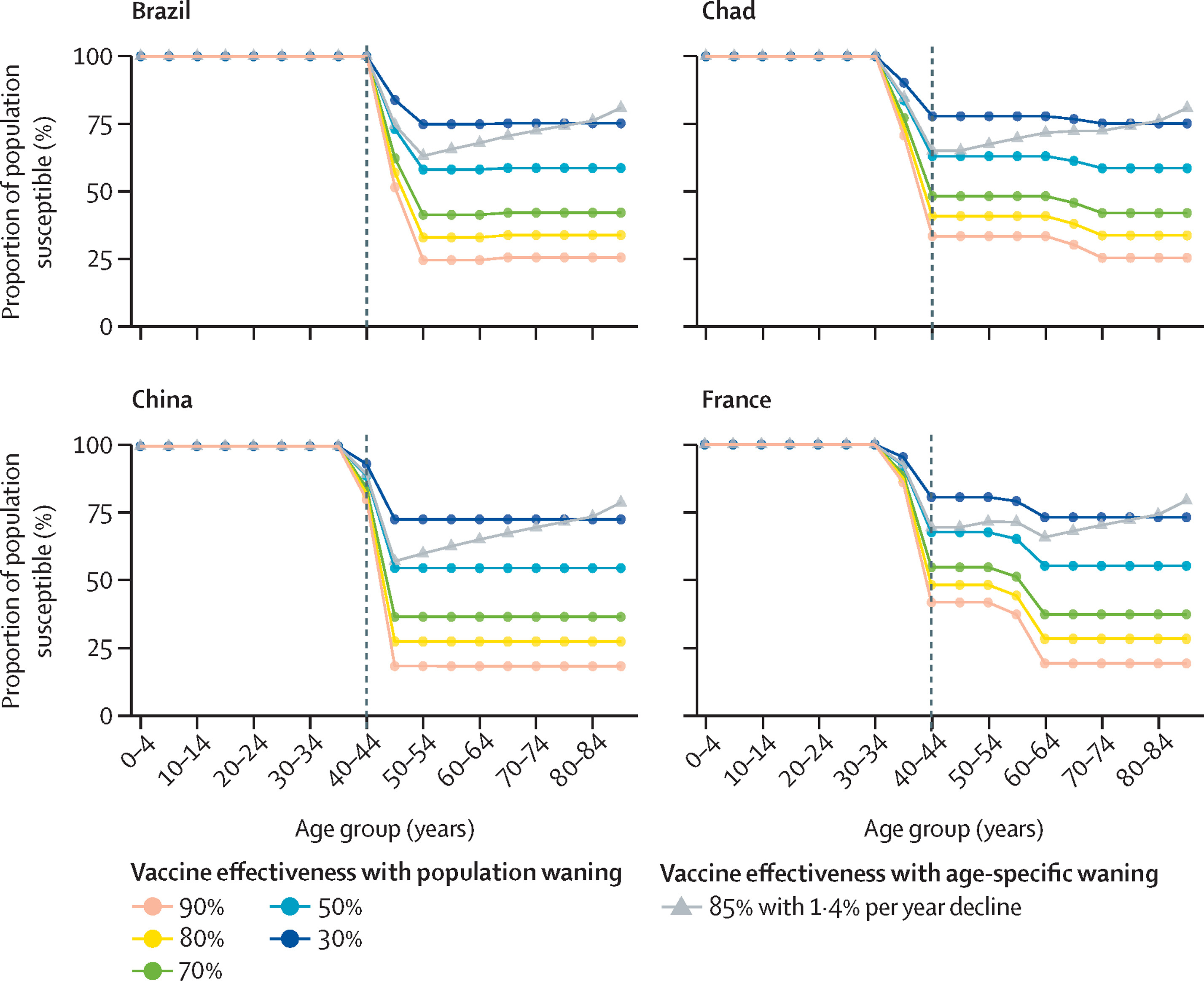
Our understanding of the exact effectiveness of the smallpox vaccine against monkeypox remains incomplete, hence our focus on the relative geographic distribution of vulnerability. We explored how differing effectiveness and waning patterns would affect current mpox susceptibility estimates (see figure above).
These estimates are for susceptibility to mpox disease. Data on how protective smallpox vaccine is for mpox infection and onward transmission are limited (but expected to be high). So our estimates should be interpreted for susceptibility to symptomatic disease.
These are population vaccination coverage estimates so are averaged over all in a population. We assume individual susceptibility to be dichotomous in our susceptibility analyses, with unvaccinated indivs vulnerable to disease + vaccinated indivs protected. But individual protection can vary based on health, revaccination, etc.
Indiv susceptibility is also predicted based only on current age & country-specific smallpox vaccination cessation and coverage. So if you were not vaccinated before cessation, < 100% coverage might explain this. If you were vaccinated after cessation, surplus vaccine supply might.
Finding country-specific data from incomplete historical records brings inherent uncertainty to our estimates. We borrow information geographically where available and carry out an uncertainty analysis to show that overall estimates are robust to known uncertainties.
We also hope that this can become a living database. You can check out your own country’s data at our Github repo, and help improve our national estimates of smallpox vaccination cessation and coverage near cessation.
Last note on the 2022 mpox crisis: current observations suggest transmission is dominated by contact processes in clustered social networks. So predicting potential widespread mpox transmission would require considering contact patterns, mobility & real-time prevalence, alongside susceptibility.